IGF-1 LR3 vs HGH: Which Growth Enhancer Is Better?

The decision to use IGF-1 LR3 or HGH (somatropin) is like deciding between two sides of the coin. Both activate the growth-hormone/IGF – 1 pathway, but they get into the body differently. HGH is a complete length hormone that imitates the hormones produced by the pituitary. IGF 1-LR3 is an insulin-like growth factor-1 lab-modified fragment with a longer half-life and better receptor binding. The former acts in an upstream direction, activating most tissues, whereas the latter acts in a downstream manner, providing a localized signal to muscle and connective tissue during remodeling.
Because of these various points of entry, the effects are different for athletes and biohackers on a daily basis. IGF-1 vs HGH? HGH typically grows fatter muscles and a slight enhancement in recovery, and IGF-1 LR3 is appreciated on account of richer pumps and enhanced rapidity of nutrient division. The two compounds are not able to substitute hard training, sleep, and adequate protein.
This guide eliminates the hype, clarifies actual mechanisms, contrasts advantages, portion, and side-effect profile, and concludes with a definite checklist. It will make you make the right choice-or make you decide that you do not need either at the moment.
What Is HGH (Human Growth Hormone)?
The secretion of human growth hormone occurs in pulses, the maximum being reached during deep sleep. It is administered subcutaneously as recombinant somatropin clinically.
To athletes, the attractiveness of HGH is in three aspects:
Tissue repair: It increases the rate of collagen turnover, which may reduce the stress in the tendons or ligaments during increased volume training.
Body-fat processing: During the long run, somatropin shifts metabolism to use fats as an energy source, but the ultimate result depends on diet and activity.
Feel of recovery: A good deal of users reports deeper sleep and more complete sessions, which must be attributed to fluid redistribution and glycogen refueling.
Medicine is administered in very small daily doses, which are tailored individually by the IGF-1 labs. Bigger amounts are used in physique circles, but doses that are too high too soon results in water retention, dead hands and numbed joints – signs that the recovery edge is being pushed too far into overkill. After all, HGH is a general hormonal stimulator, its efficacy is pegged on regular habitual self-discipline, rather than using the pen to its full extent.
What Is IGF-1 LR3 and How It Differs from HGH
IGF-1 LR3 is a synthetic analog of insulin-like growth factor 1 with two major changes: an added 13-amino-acid extension (“LR3”) and substitution of a single amino acid that reduces its binding affinity to IGF binding proteins. The outcome is a peptide remaining active not over minutes, but rather hours, and directly interaction with the IGF receptors in muscle and satellite cells. It does not go through the pituitary, like HGH it does not give an upstream hormone burst, and no systemwide impetus. It is a downstream stimulus directed at repairing and growing tissues.
Practically, that means:
- Quicker effect: Customers can experience enhanced pumps within a few days, not weeks.
- Specific effect: Reduced influence on water homeostasis or even glucose variability over high dose HGH- however, localized swelling close to inoculation sites may take place along with an increase in appetite.
- More intense cycles: More common are 4-6 week cycles, usually take place in post-workout or split into micro-doses both before and after training.
IGF-1 vs HGH – The Biological Connection
Both drugs sit on the same signaling highway but at different on-ramps:
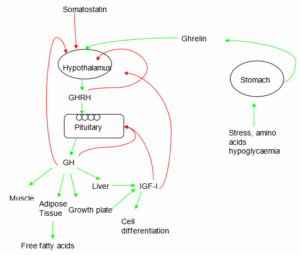
- HGH → Liver → IGF-1: HGH pulses stimulate the liver (and tissues) to produce endogenous IGF-1, raising systemic levels slowly and broadly.
- IGF-1 LR3: Skips the liver step, delivering the activity directly to receptors with a longer active window.
Think of HGH as the master switch that lights up multiple rooms, while IGF-1 LR3 is a spotlight pointed at the hypertrophy corner. Both can be used to enhance growth, but there is a difference in how they are used, the side effects and the ideal application use case of each. That’s since one floods the whole circuit, and the other is used to target a specific outlet.
IGF-1 vs HGH – Mechanism of Action in the Body
Both of the compounds would be on the same growth-axis highway, but they will have different ramps and would cause different traffic trends.
HGH (somatropin)
- Pituitary signal: Injected HGH mimics the hormone your pituitary pulses at night.
- Liver relay: The liver responds by releasing systemic IGF-1 plus dozens of secondary growth factors.
- Broad sweep: Those factors circulate everywhere – muscle, bone, cartilage, even fat cells – creating a diffuse, whole-body effect.
IGF-1 LR3
- Direct hit: This is a long-acting IGF analog that bypasses the liver-pituitary-loop and goes directly to the IGF-1 receptors of muscle and connective tissue.
- Increased half-life: Chemical modifications increase the duration of activity by several hours (when compared to minutes (native IGF-1)) keeping the receptors active during the post-workout window.
- Limited scope: Since it does not act through growth-hormone receptors, there will be minimal collateral effects, such as water retention, general metabolic changes.
IGF-1 vs HGH – How Fast Do They Work?
- HGH: Prolonged users normally notice the benefits such as fuller muscles and restful sleep in 3–4 weeks. The corresponding time of systemic IGF-I increment and tissue remodelling is the same as that delay.
- IGF-1 LR3: The pump effect and nutrient segregation can be optimally enhanced in days since the peptide is direct-acting and does not depend on liver metabolism. A number of lifters get denser workouts by week 1.
It is not all about speed, though. The slower onset of somatropin tends to provide a wider, long pay-off, whereas IGF-1 LR3 is a fast, narrow blast over a shorter duration of block-degree such as recomposition.
IGF vs HGH – Benefits and Results
Overlap: Both compounds aim at the GH–IGF-1 axis, so shared outcomes include better tissue repair, improved workout recovery, and a tilt toward leaner body composition when nutrition is on point.
| Category | HGH (systemic driver) | IGF-1 LR3 (targeted driver) |
| Muscle fullness | Gradual, steady; tied to glycogen & water shifts | Quick, workout-specific pumps |
| Connective-tissue support | Broad collagen turnover over months | Local satellite-cell activation; helpful for lagging muscle groups |
| Fat-loss assist | Encourages lipolysis during long cuts | Indirect; mainly via better nutrient partitioning |
| Sleep & recovery feel | Often deeper sleep, smoother recovery blocks | Minimal sleep impact; faster post-session “reset” |
| Side-effect radius | Water retention, joint puffiness at high doses | Injection-site swelling, appetite spikes; less systemic bloat |
To conclude about IGF 1 vs HGH: Use HGH when you want a long-term foundation – off-season mass or extended recomp. Reach for IGF-1 LR3 when you need a short, sharp edge: peak weeks, stubborn muscle activation, or a bridge between larger cycles.
IGF-1 LR3 vs HGH for Muscle Growth
- IGF-1 LR3: Local hypertrophy blocker. Post-workout or directly into a leading up muscle micro-dose may increase satellite-cell activity and protein synthesis directly in the area of stimulus. It is commonly used with high-rep finishers by the users to fix the flow of nutrients.
- HGH: Master of accrual on a global level. It allows you to add progressively heavy systemic IGF-1 to the body and fortify connective tissues so that you can add months of heavy work without feeling pounded.
They are sometimes sequenced in smart programs: HGH as a base period over the year, followed by bursts of 4–6 weeks of IGF-1 LR3 in areas that are difficult to fat. Anyhow, the same triad benefits include progressive overload, enough protein, and regular sleep.
IGF-1 and HGH for Fat Loss and Metabolism
Both components work in one direction of the way your body maintains insulin balance. The human growth hormone increases the levels systemically, which controls the lipolytic enzymes and makes the body burn more fat, particularly when under a calorie deficit with regular cardio or step goals. Generally, pinch-able fat mass decreases slowly and steadily over months, with a slight bloating of the muscles because of the glycogen and water realignment.
IGF-1 LR3 acts in a lower manner. It can control most of each meal towards a muscle cell repair and less towards fat storage by enhancing nutrient partitioning at the muscle cell. Pumps become heavier, and carbohydrate being used after exercise can be taken in a lot more readily, so the cleanliness of refeeds is increased when cut.
P.S. No one of these compounds is more alluring than the poor diet discipline.
IGF-1 vs HGH – Dosage, Administration, and Duration
HGH regimens typically are based upon the daily subcutaneous injection.
- The recreational athletes begin with low doses of about one to three IU, and they maintain the doses over three to four weeks, after which they may then have small increments. The higher doses (four to six IU) are used in those who have years of progressive overload experience behind them, since the potential for side effects increases rapidly.
- The majority remain twelve to twenty-four weeks to allow the systemic IGF-1 upsurge and connective tissue to get acclimatized. Regularity in time, typically in the morning or before sleeping aids in monitoring outcomes and water balance.
The dosage of IGF-1 LR3 is expressed in micrograms and not IU.
- The usual dosage is 20-50 mcg with each injection, administered five days a week during four to six weeks. To sustain the engagement of receptors during the anabolic window, many athletes divide the amount in half, half prior to exercise and the other half after exercise.
- The intramuscular injection is normally used in the muscle area near the muscle being trained in order to focus on a specific area, although the sub-Q is used when rotation of the site is a problem.
- IGF-1 LR3 has a low affinity to binding receptors, and therefore its long half-life already provides sufficient exposure; exceeding 50 mcg does not produce additional effects and growth and results in spikes of appetite or localized edema.
Development of a cycle is reduced to objectives. Long and steady background support? Choose HGH. Incidental recomposition or determined-lazy muscle fix? IGF-1 LR3 fits better.
You can decide between IGF 1 vs HGH, but whichever you choose, keep a track of morning weight, waist, photos, and joint feel even before you consider increasing the dose.
Can You Combine IGF-1 and HGH Together?
Yes, but synergy isn’t automatic. Because HGH elevates systemic IGF-1 and IGF-1 LR3 adds a direct receptor hit, stacking can overshoot the pathway and amplify water retention, hand numbness, and blood-glucose swings.
Most lifters who blend them do so in a tiered approach: a modest daily somatropin baseline paired with very small IGF-1 LR3 pulses (10–20 mcg) around key workouts. Even then, they schedule short overlap windows – four weeks on, at least four weeks off – to reassess markers and side effects.
Key safeguards: rotate sites to avoid scar tissue, keep sodium and carbs consistent, and set hard stop signs – persistent wrist tingling, facial puffiness, fasting glucose creeping upward. If those appear, drop the LR3 first before touching the HGH base.
Remember that progressive overload, solid protein distribution, and eight hours of sleep still drive the bulk of your progress; peptides should fine-tune the process, not replace the fundamentals.
Side Effects and Safety
Even though both compounds target the same growth pathway, they present different risk profiles. HGH raises growth hormone and downstream IGF-1 everywhere, so systemic side effects show up first.
The most common are soft-tissue water retention, morning hand swelling, carpal-tunnel–like tingling, and joint stiffness around the wrists and knees. Higher doses can bump fasting glucose or blood pressure, especially if sleep or carb timing is erratic. Headaches or ankle edema are early signals you’re pushing beyond your current tolerance.
IGF-1 LR3 delivers a tighter, shorter pulse, so problems tend to be local: redness or a “welt” at the injection site, temporary appetite spikes, or mild hypoglycemia if you pin fasted and then delay eating. Because it bypasses the pituitary, global bloat is less common, but abusing high microgram counts can still desensitize receptors, giving you flat workouts and dull pumps.
Rotate sites, keep sodium and water steady, and track morning grip strength to spot issues before they escalate. If fingers feel numb on waking or waist and scale leap upward, take a deload or drop dosage. Blood work – IGF-1, fasting glucose, lipids – every eight to twelve weeks provides a reality check mirrors can’t.
Which One Is Safer – IGF-1 or HGH?
IGF-1 LR3 is best for fast physique changes. HGH supports long-term recovery, wellness, and overall resilience.
On paper, IGF-1 LR3 carries the lighter systemic burden because it skips the pituitary and works for only a few hours, limiting water shifts and glucose swings. Most problems stay local – small welts, short-lived appetite rushes – so dialing dose and injection technique usually fixes them.
HGH, by contrast, raises multiple downstream hormones for twenty-four hours or more; that broad reach is why hand edema, joint aches, and insulin resistance appear when doses climb. Yet, safety really comes down to context.
Moderate HGH plus regular labs can outperform reckless IGF-1 megadosing. The safer option is the one you respect: start low, track markers, adjust slowly, and stop at the first hint of nerve tingling, uncontrolled bloat, or rising resting blood glucose levels.
Which One Should You Choose?
Your choice between IGF vs HGH should reflect your training phase, physique goals, and how fast you want to see changes. While both compounds support growth and recovery, they work best in different contexts. IGF-1 LR3 delivers faster, localized effects — ideal when you want to target muscle growth quickly. In contrast, HGH works more gradually, improving sleep, skin, joint health, and fat metabolism over time. Here’s a quick guide:
| Goal | Recommended Option | Why This Choice Works |
| Bodybuilding (mass) | IGF-1 LR3 | Fast-acting, targets muscle directly, ideal for hypertrophy cycles. |
| Cutting / Fat loss | HGH | Promotes fat-burning, maintains lean mass, supports metabolic health. |
| Recomp / Lean gains | Stack (HGH + IGF-1) | Balances fat loss with lean tissue gain when diet and training are tight. |
| Wellness / Anti-aging | HGH | Improves sleep, recovery, skin, and long-term physiological balance. |
| Injury recovery / soft tissue | IGF-1 LR3 or IGF-1 DES | Speeds up local repair and supports tissue regeneration. |
IGF1 vs HGH: Final Verdict
HGH is the long-game quarterback; IGF-1 LR3 is the quick-strike wide receiver. Use HGH when you want a steady hormonal backdrop that makes hard training sustainable for months and quietly improves body composition. Deploy IGF-1 LR3 in short bursts to light up lagging muscle or sharpen a recomp phase without as much systemic baggage. Mixing both can work, but only with conservative doses, clear stop signals, and rock-solid fundamentals. If sleeves are tight, but joints ache, you aimed too high; if training flies and labs stay tidy, you chose well. The axis should serve your program, not dictate it alone.